

Dissociation in Children and Adolescents: Understanding Protection Through a Play Therapy Lens
Written By: Holly Dudley, Resident in Counseling, NCC & Samantha Long, PhD, LPC, RPT, NCC
How trauma, overwhelming experiences, and disconnection can shape children’s emotions, nervous systems, relationships, and the ways they communicate what feels too big for words.

Dissociation in children and adolescents can be hard to recognize. It does not always look dramatic. It does not always look like a child is completely “gone” or unaware of what is happening around them. Sometimes it looks like a child who suddenly goes quiet. Sometimes it looks like a teen who keeps saying, “I don’t know,” even when they seem like they should be able to answer. Sometimes it looks like silliness, sleepiness, numbness, confusion, zoning out, shutting down, forgetting, freezing, or seeming far away even while sitting right in front of us.
Sometimes it shows up in the playroom through sudden shifts in energy, repeated scenes that do not resolve, characters who disappear or hide, intense fantasy, changes in voice or role, or play that feels disconnected, fragmented, or hard to follow. What may look like avoidance, resistance, or “checking out,” may actually be a protective adaptation. For caregivers, these moments can be confusing. For clinicians, they can be easy to miss. For children and adolescents, these moments may not feel like a choice at all. When a young person has experienced complex trauma, chronic stress, attachment disruption, or overwhelming emotional experiences, dissociation can become one way the nervous system protects them from what feels too big to hold all at once.
This does not mean every child who zones out is dissociating. It does not mean every teen who shuts down has a dissociative disorder. It does not mean we need to rush toward labels. But it does mean we need to understand disconnection with more curiosity, care, and clinical depth. In play therapy, these protective responses often speak through the child’s body, roles, themes, stories, silence, movement, and relationship with the therapist. This is part of why dissociation in children and adolescents requires a developmentally sensitive approach. Children do not always explain what is happening inside of them directly. They often show us through play, behavior, and connection.
*Our upcoming training, Working with Dissociative Kids and Teens in Play Therapy, is going to help clinicians better understand complex trauma, dissociative responses, ego states work, and developmentally appropriate play therapy interventions for children and adolescents.
Before we can support healing, we have to understand what protection may look like.
What is Dissociation? Understanding It as a Spectrum
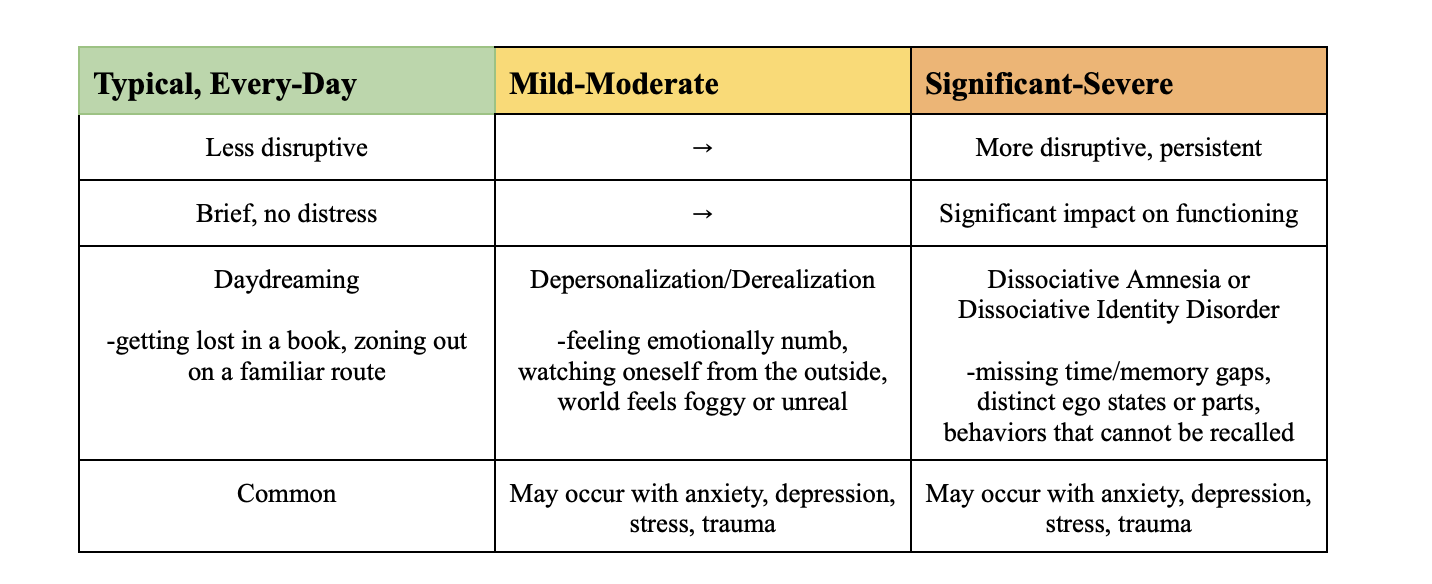
Dissociation is not a single, fixed experience. It exists on a spectrum, ranging from everyday, typical experiences of disconnection to more significant disruption in awareness, identity, memory, and sense of self. At the milder end of the spectrum, dissociation can look like everyday absorption: getting lost in a book, music, video game, or zoning out. These experiences are common and do not indicate pathology. The nervous system creates momentary distance from the present moment, and the person drifts and then returns, often without distress. Further along the spectrum, dissociation may involve more persistent experiences of detachment. A child may feel “numb” or emotionally flat during stressful situations. A teen might feel like they are watching themselves from a distance, almost like an observer of their own life. They may feel that the world around them does not quite feel real, or that they themselves do not feel real. These experiences are often described in clinical literature as depersonalization (feeling detached from oneself) and derealization (feeling detached from one’s surroundings). At the more significant end of the spectrum, dissociation may involve persistent disruptions in memory, identity, or functioning and these responses may meet criteria for a formal dissociative disorder.
The key clinical question: not simply whether a child dissociates but → how often, under what circumstances, does it interfere with safety, relationships, learning, development, and ultimately, what is it serving?
When the Nervous System Adapts
Dissociation does not only happen in children who have experienced trauma. Any young person whose nervous system is regularly working hard to manage overwhelming internal experiences may develop dissociative responses over time. For some children, that overwhelm comes from chronic anxiety, a nervous system that is often activated, braced, or on high alert. For others, it comes from depression, emotional numbness, or a persistent sense of disconnection from themselves and the world around them. For others still, it comes from attachment stress, relational unpredictability, or simply not yet having the co-regulation and developmental support needed to process big feelings. For some children, dissociation does emerge in the context of complex trauma, exposure to overwhelming experiences, often in relationships where the child should have been able to find safety (National Child Traumatic Stress Network, n.d.). When that is the case, the nervous system may organize around survival in ways that later interfere with connection, regulation, learning, and healing.
Diseth and Christie (2005) described dissociation as a process where experience becomes fragmented into pieces: sensations, thoughts, feelings, and perceptions held separately rather than integrated as a whole. When something is too intense to process all at once, memory may be held in pieces. This helps explain why children and teens may not always be able to tell a clear story about what happened, even when their body, behavior, play, or emotions are still carrying parts of their experience.
It is also why dissociation is so easily misread. A child who is overwhelmed may look like they are ignoring their teacher. A teen who is disconnected may look like they do not care. A child who cannot access words may look defiant. Diseth and Christie (2005) noted that dissociative symptoms are frequently mistaken for anxiety, attention difficulties, conduct concerns, mood shifts, or even psychosis, and that children may have a greater tendency and capacity for dissociation than adults, with some imaginative and fantasy experiences being developmentally typical (Diseth and Christie, 2005). A young child’s rich fantasy life is not automatically a sign of trauma. But, at the same time, capacity for absorption can, in the context of chronic stress or overwhelming experience, become a survival strategy that deserves clinical attention. This is not a reason to assume dissociation is always present, but it is a reason to stay curious when a child’s presentation feels confusing, inconsistent, or hard to understand through one lens alone.
Dissociation, wherever it falls on the spectrum, is not a behavioral problem or a character flaw. It is an adaptation. Understanding what it is adapting to is where meaningful support begins.
Why This Looks Different in Children and Adolescents: Signs to Know
Because children are still developing their language, identity, and emotional awareness, dissociation in young people does not always announce itself clearly. It often looks like something else entirely.
What Dissociation May Look Like In Children
For children, dissociation can be especially difficult to identify because children often lack the language to describe internal experiences of unreality, detachment, or discontinuity. Instead of reporting how they feel, they show us through behavior. Children may not say:
“I feel far away from myself”
“I do not feel real right now”
“A part of me is scared”
“I shut down when I feel too close to someone”
“I cannot stay present when my body remembers something painful.”
But they may show us. They may show us through a character who hides. A figure who freezes. A story that repeats. A baby who needs rescuing. A villain who takes over. A protector who will not let anyone close. A scene that keeps ending before repair can happen. A sudden shift in tone, posture, energy, or role.
Signs in younger children may include:
Glazed or blank look in their eyes, sometimes described by caregivers as “the lights are on but nobody’s home.”
Appearing to “snap out” of something and then returning to the present moment without awareness of how much time has passed.
Sudden unexplained shifts in mood, behavior, or energy that seem inconsistent with what just happened.
Not responding to their name being called even when they are not asleep and appear to be awake.
Describing themselves in the third person.
Play that feels fragmented, chaotic, or repetitively stuck; themes that cycle without resolution.
Sudden freezing or going very still in response to what appears to be a mild or neutral trigger.
These signs can be easy to miss or explain away as “just being tired,” “just being dramatic,” or “just acting out.” That is why clinical curiosity and developmental attunement matter.
What Dissociation May Look Like in Adolescents
Adolescents may have more language than younger children, but they do not always have the words for dissociation or the safety and trust required to disclose internal experiences that may feel confusing, frightening, or shameful.
Signs in adolescents may include:
Describing feeling like they are watching themselves from the outside (observing their own life from a distance).
Reporting that the world feels “unreal,” “dreamlike.”
Significant memory gaps (missing time they cannot account for, or not remembering events other say happened).
Finding evidence of things they said, wrote, or did that they have no memory of.
Sudden personality or behavioral shifts that feel jarring or out of character, even to the adolescent themselves.
Emotional numbing or flatness, particularly in situations where emotion would be likely.
A pattern of “zoning out” in therapy, school, and at home.
Difficulty staying present during sessions even when appearing engaged.
Because adolescents are often aware of stigma around mental health and may fear being seen as “crazy,” they may minimize, dismiss, or hide these experiences. Clinicians working with adolescents need to hold these signs with curiosity and without rushing to conclusions in either direction.
Play Therapy is a Developmentally Appropriate Approach
A developmentally appropriate approach like play therapy allows children to express experiences that may be difficult, or impossible, to put into words. Through play, art, sand, movement, storytelling, fantasy, and the therapeutic relationship, children can communicate emotions and experiences that feel fragmented or overwhelming. Rather than interpreting or directing the play, the therapist remains attuned, curious, and responsive, allowing the child's inner world to unfold at their own pace. As Wieland (2015) noted, understanding dissociation involves more than recognizing its symptoms; clinicians must also understand how dissociation emerges within the therapeutic relationship and how it shapes the child's interactions in the playroom.
Unlike adults, children often process their experiences through action, symbolism, imagination, and relationship before they can organize them into language. Play creates a sense of emotional distance that allows children to approach difficult experiences in ways that feel manageable rather than overwhelming. Within the safety of a consistent therapeutic relationship, children can revisit themes of fear, protection, control, loss, or connection without needing to talk about them directly. Over time, these experiences can support increased emotional regulation, flexibility, integration, and a greater sense of safety within themselves and in relationships.
Children experiencing dissociation may communicate through themes of protection, danger, hiding, rescue, control, separation, transformation, or survival. Play may become repetitive, chaotic, disconnected, or highly organized around safety. These patterns are not problems to eliminate but meaningful forms of communication that help guide therapeutic understanding while honoring the child's pace.
Research suggests there is no single treatment model for dissociation in children and adolescents. Instead, interventions such as play therapy, art therapy, family therapy, EMDR, cognitive and behavioral approaches, and other trauma-informed treatments may all play a role (Diseth & Christie, 2005). For many children, play provides a bridge between overwhelming experiences and the safety needed to begin organizing, expressing, and integrating them.
Looking Beyond the Behavior
Whether you are a parent, caregiver, educator, or mental health professional, one of the most important shifts we can make is moving from asking, "What's wrong with this child?" to asking, "What might this child be protecting themselves from?" Dissociation is not a sign that a child is broken. More often, it reflects a nervous system that has found a way to survive experiences that felt overwhelming. When we begin to understand these responses through a developmental, relational, and trauma-informed lens, behaviors that once seemed confusing often begin to make sense. Through safety, attunement, and developmentally appropriate interventions such as play therapy, children do not have to remain disconnected forever. Healing is not about taking away protective responses before a child is ready; it is about helping them discover that, little by little, they no longer need those protections in the same way.
Every behavior tells a story. Sometimes, play gives children the words they have not yet found.
Join Us
Working with Dissociative Kids and Teens in Play Therapy
July 17th 9am - 12:15pm 3 APT approved credits
This training is appropriate for mental health professionals, play therapists, and clinicians supporting children and adolescents impacted by complex trauma, dissociation, attachment disruption, and trauma-related protective responses.
To learn more or register, visit: https://www.eventbrite.com/e/working-with-dissociative-kids-and-teens-in-play-therapy-tickets-1990915259134?aff=oddtdtcreator
References
National Child Traumatic Stress Network. (n.d.). Complex trauma. https://www.nctsn.org/what-is-child-trauma/trauma-types/complex-trauma
Diseth, T. H., & Christie, H. J. (2005). Trauma-related dissociative (conversion) disorders in children and adolescents: An overview of assessment tools and treatment principles. Nordic Journal of Psychiatry, 59(4), 278–292. https://doi.org/10.1080/08039480500213683
Wieland, S. (Ed.). (2015). Dissociation in traumatized children and adolescents: Theory and clinical interventions (2nd ed.). Routledge.